
How Olive Oil Modulates Lipid Pathways
Olive oil does more than add fat to a meal: it can shift how your body handles cholesterol, insulin, inflammation, and liver fat. The main pattern from the article is simple: standard olive oil has small effects on a basic lipid panel, but high-phenolic extra virgin olive oil (EVOO) does more for LDL oxidation, HDL function, insulin response, and blood vessel health.
Here’s the short version:
- Oleic acid helps cells handle fat and insulin better.
- Polyphenols such as hydroxytyrosol and oleuropein help cut oxidative stress and calm inflammatory signals.
- In human research, an EVOO-rich Mediterranean diet was tied to a 51% lower rate of type 2 diabetes.
- Intake of at least 1/2 tablespoon per day was linked to 15% lower cardiovascular disease risk and 21% lower coronary heart disease risk.
- Standard cholesterol changes are often small unless olive oil replaces butter or other saturated fats.
- The strongest effects tend to come from high-phenolic EVOO, not just “more oil.”
If I boil the article down to one idea, it’s this: olive oil seems to work best when it is extra virgin, high in phenolics, and used in place of saturated fat. That’s where the clearest shifts show up in lipid handling, LDL protection, HDL behavior, insulin signaling, and inflammation.
Before the article gets into the studies and pathways, that’s the main takeaway you need.
Olive Oil Raises LDL and Increases Fat Cells?! (new study)
sbb-itb-4066b8e
How Olive Oil Affects Core Lipid and Insulin Signaling Pathways
Three pathways explain most of olive oil's metabolic effects: PPAR signaling, IRS-PI3K-Akt insulin signaling, and NF-κB-driven inflammation.
PPAR, SREBP, and Genes That Control Fat Oxidation and Lipid Storage
PPARs are nuclear receptors that help direct fat oxidation, lipid storage, and glucose handling. Hydroxytyrosol (HT) boosts the expression of PPAR-α and PPAR-γ in adipocytes, while oleic acid acts as a direct PPAR ligand. Together, they blunt the TNF-α-driven drop in PPAR-γ.
In animal models, HT supplementation at 10 mg/kg/day increased hepatic PPAR-α expression and FGF21, which improved insulin sensitivity. In plain English, these receptor changes push cells more toward burning fat and less toward storing it.
HT also blocks the SREBP2/PCSK9 pathway, which may help LDL receptor activity and LDL clearance. A randomized human trial found that HT plus punicalagin inhibited this pathway and increased LDL clearance.
IRS-PI3K-Akt Signaling and Insulin Sensitivity
Olive oil doesn't just act through nuclear receptors. It also affects insulin receptor signaling.
Here's the basic chain: IRS → PI3K → Akt. When this pathway works well, cells can take up glucose more easily.
Oleic acid, the main monounsaturated fat in olive oil, supports this pathway directly. In vitro studies show that it increases the expression of IRS1 and the p110β catalytic subunit of PI3K, while lowering the p85α regulatory subunit. That matters because a lower p85α/p110β ratio improves insulin signaling.
Palmitic acid pushes things the other way. It increases the p85α/p110β ratio and lowers IRS1 expression, which promotes insulin resistance. Human data point in the same direction: lower IRS1 expression has been found in visceral adipose tissue, and oleic acid was inversely correlated with p85α.
NF-κB, Oxidative Stress, and Lipid-Driven Inflammation
Olive oil's effects also reach inflammatory signaling. EVOO polyphenols, especially ligstroside aglycon and hydroxytyrosol, suppress NF-κB, MAPKs, and JAK2/STAT3.
Human trials also link EVOO phenolic compounds with lower systemic inflammatory markers, including IL-6 and C-reactive protein, along with reduced expression of CD40 ligand. That last effect may help limit oxidative damage to LDL particles.
What Studies Report on Cholesterol, Triglycerides, and Lipoprotein Function
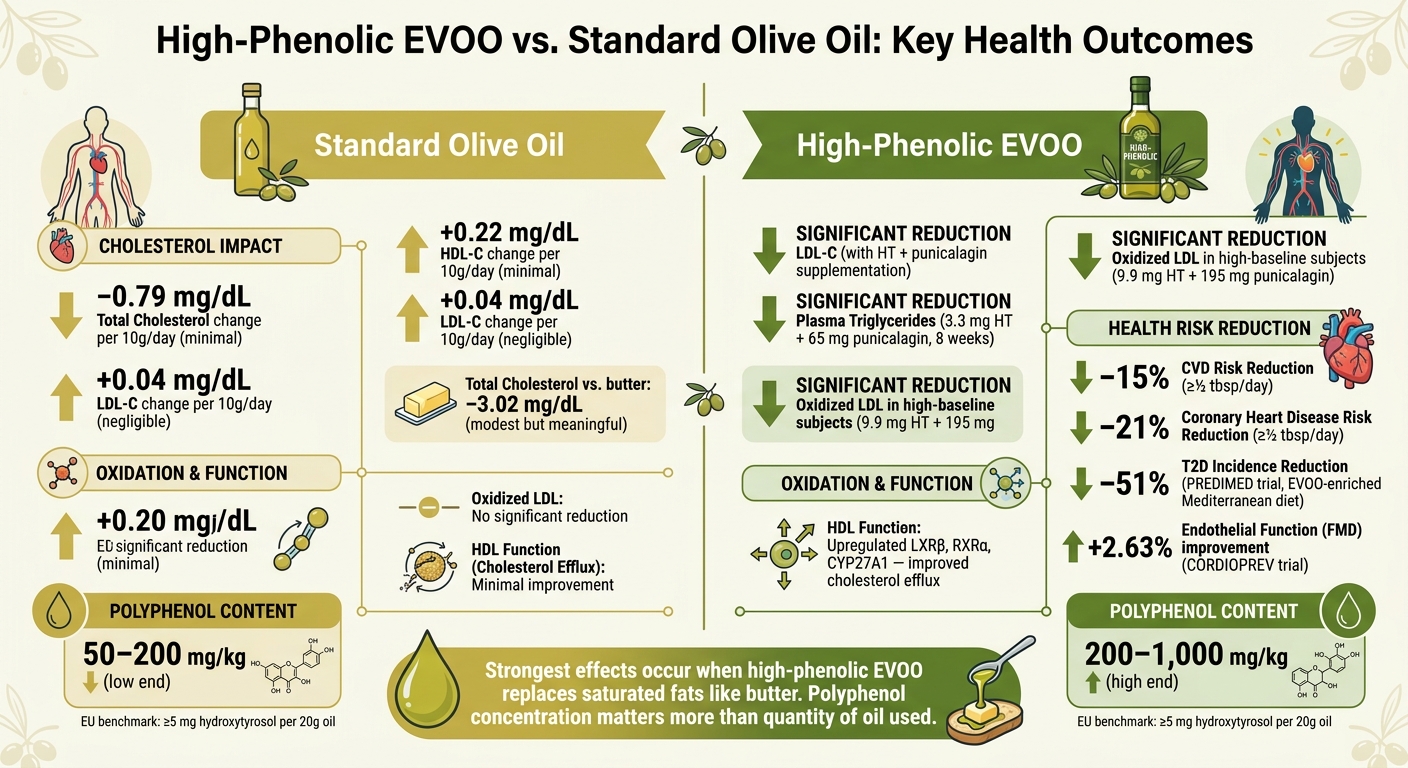
High-Phenolic EVOO vs. Standard Olive Oil: Key Health Outcomes
Average lipid changes from olive oil tend to be small. The clearer effects usually show up with polyphenol-rich EVOO and when olive oil replaces saturated fat. In human trials, that pattern shows up again and again: standard lipid markers may shift a little, while lipoprotein function often shows a clearer response.
Changes in LDL-C, HDL-C, and Triglycerides
A meta-analysis of 34 randomized controlled trials with 1,730 participants found that each extra 10 g/day of olive oil led to only tiny changes in standard lipids. Total cholesterol changed by about 0.79 mg/dL, LDL-C by 0.04 mg/dL, and HDL-C by 0.22 mg/dL. Put plainly, olive oil on its own doesn't seem to move a standard lipid panel very much.
The picture changes when olive oil replaces butter. In that case, serum total cholesterol fell by about 3.02 mg/dL. That's still a modest change, but it matters more because the swap removes a source of saturated fat.
Trials using polyphenol-rich compounds show stronger effects. In hypercholesterolemic subjects, daily supplementation with 3.3 mg hydroxytyrosol (HT) plus 65 mg punicalagin for 8 weeks led to significant reductions in both plasma triglycerides and LDL-C. So the clearest lipid effects tend to appear in higher-risk groups and with higher-polyphenol interventions.
These small shifts in LDL-C, HDL-C, and triglycerides matter most when they also affect oxidation and HDL behavior.
Oxidized LDL and HDL Function
Looking past the usual cholesterol numbers, EVOO may improve how lipoproteins act. Two findings stand out.
The first is oxidized LDL. In one 8-week trial using 9.9 mg HT combined with 195 mg punicalagin, ox-LDL fell significantly, but only in participants who started with high baseline levels. That makes sense: the effect was strongest in the people who had more oxidation to begin with.
The second is HDL function. This is where things get more interesting. HDL-C by itself doesn't tell the whole story, because cholesterol efflux is a better marker of anti-atherogenic activity.
In the VOHF trial, a randomized, double-blind, crossover study of 22 hypercholesterolemic volunteers, participants consumed 25 mL/day of a phenol-enriched virgin olive oil at 500 mg/kg total. After 3 weeks, researchers found significant upregulation of LXRβ (p = 0.005), RXRα (p = 0.005), and CYP27A1 (p = 0.041), which are genes involved in moving cholesterol out of macrophages into HDL particles. So even when HDL-C barely changes, HDL may still work better.
Comparison Table: Olive Oil Type, Study Population, Duration, and Lipid Outcomes
The studies below separate standard olive oil effects from higher-polyphenol interventions.
| Olive Oil Type / Intervention | Study Population | Duration | Key Lipid & Lipoprotein Outcomes |
|---|---|---|---|
| Phenol-enriched VOO (500 mg/kg olive + thyme phenols) | Hypercholesterolemic adults | 3 weeks | Upregulated CYP27A1, LXRβ, ABCA1; increased cholesterol efflux |
| HT (3.3 mg) + Punicalagin (65 mg) | Hypercholesterolemic adults | 8 weeks | Significant reduction in plasma triglycerides and LDL-C |
| HT (9.9 mg) + Punicalagin (195 mg) | Healthy adults | 8 weeks | Reduced ox-LDL in subjects with high baseline levels |
| Standard olive oil (meta-analysis, 34 RCTs) | General adults | 3 weeks–3 years | Trivial changes in total cholesterol, LDL-C, HDL-C vs. other plant oils; meaningful total cholesterol reduction vs. butter |
High-polyphenol EVOO, especially when it replaces saturated fats, shows effects both on a lipid panel and in the way lipoproteins function at the molecular level.
How These Lipid Effects Connect to Metabolic Health
These lipid changes don’t just look good on a lab report. They may also help cut oxidative stress and inflammation, two big drivers of insulin resistance, metabolic syndrome, and cardiovascular disease. And the same signaling pathways don’t stop in the bloodstream. They also affect the liver and fat tissue.
Insulin Resistance, Metabolic Syndrome, and Liver Fat
Hydroxytyrosol and oleuropein appear to support glucose control through pathways such as AMPK, NF-κB, GLP-1, and DPP-4. One of the clearest human examples comes from the PREDIMED trial. In that study, a Mediterranean diet enriched with EVOO was linked to a 51% reduction in type 2 diabetes rates compared with a low-fat diet. It also delayed the use of glucose-lowering drugs and reduced insulin starts by 12% in people with type 2 diabetes.
The blood sugar picture is a bit mixed, though. Post-meal glucose tends to improve most often, while fasting glucose and HOMA-IR findings are less consistent. The pattern seems stronger in people who already have metabolic risk, which makes sense. When someone is already off track, there’s often more room for change.
In the liver, the clearest signal is lower fat buildup. EVOO polyphenols appear to support fatty acid oxidation through hepatic PPAR-α and FGF21, which may help reduce hepatic fat. In a 4-month randomized, double-blind, placebo-controlled trial of 80 adolescents with non-alcoholic fatty liver disease (NAFLD), a mix of 7.5 mg hydroxytyrosol and 10 mg vitamin E led to a significant drop in steatosis grade, insulin resistance, and triglyceride levels.
Body Weight, Fat Distribution, and Cardiometabolic Risk
These same metabolic effects may also carry over to body fat distribution and vascular risk. In one study of overweight women, taking 5–15 mg of hydroxytyrosol per day led to significant reductions in body weight and visceral fat within 4 weeks.
For cardiometabolic risk, the evidence is steadier. Daily intake of at least half a tablespoon of EVOO is linked to a 15% reduction in CVD risk and a 21% reduction in coronary heart disease (CHD) risk. That’s a pretty strong signal for a simple food habit.
The CORDIOPREV trial, a long-term randomized study in patients with established coronary heart disease, found that a Mediterranean diet rich in EVOO improved Flow-Mediated Dilation (FMD) by 2.63% compared with a low-fat diet. That matters because FMD is a useful marker of endothelial health. Even small shifts in vascular markers can add up. For example, a 2 mmHg drop in blood pressure is linked to a 10% lower stroke risk and a 15% lower heart attack risk.
The table below sums up the main outcomes.
| Outcome | Evidence Level | Key Finding |
|---|---|---|
| T2D Prevention | High (Large RCTs) | 51% reduction in incidence with EVOO-enriched Mediterranean diet |
| Postprandial Glucose | Moderate (Individual RCTs) | Significant improvements, especially in at-risk populations |
| Fasting Glucose / HOMA-IR | Low to Moderate (Meta-analyses) | Neutral in most analyses; benefits appear in higher-risk groups |
| Liver Fat (NAFLD) | Moderate (Small RCTs + Animal) | Reduced steatosis grade and insulin resistance with HT supplementation |
| Endothelial Function (FMD) | Moderate (RCT) | +2.63% improvement in coronary heart disease patients |
| CVD / CHD Risk | High (Cohort + RCT) | 15–21% risk reduction with ≥½ tbsp/day EVOO |
Why EVOO Quality and Freshness Matter and What the Research Means in Practice
Polyphenol Content, Processing, and Storage
Those lipid effects only hold up if the oil still has enough phenolics to help with oxidation and inflammation. Put simply, EVOO works best when its phenolic fraction makes it through processing intact.
That’s one reason extraction method matters. EVOO is mechanically extracted, which helps keep more phenolics in the oil. Refined olive oil loses many of them during refining.
Polyphenol content can vary a lot, from about 50 to 1,000 mg/kg, based on cultivar, ripeness, and handling. And that difference isn’t just a lab detail. In a 2025 trial, 8 g/day of high-phenolic EVOO lowered total cholesterol more than 20 g/day of lower-phenolic EVOO, even though polyphenol intake was similar. So the concentration of phenolics seems to matter more than simply using more oil.
Storage matters too. Even high-phenolic EVOO can lose activity if it’s handled badly. Heat, oxygen, and light break down phenolics, which is why studies store EVOO in dark glass at 59–64°F (15–18°C). One practical benchmark is 5 mg of hydroxytyrosol and derivatives per 20 g of oil, which is the minimum needed for the EU health claim.
Big Horn Olive Oil in the Context of This Research
Seen through that lens, harvest speed and storage practices aren’t just nice selling points. They can affect whether the oil still delivers the effects studied in research.
Big Horn Olive Oil says its oils are cold-pressed within 2 hours of harvest and sold within 3 months. It also offers Coratina EVOO, a cultivar known for high phenolic content.
Conclusion: Main Mechanisms and What They Mean
Across studies, the pattern is pretty clear: keeping polyphenols in the oil is linked with less LDL oxidation, better HDL function, and lower inflammatory markers such as IL-6 and C-reactive protein (CRP). In day-to-day terms, the strongest lipid effects are tied to fresh, high-phenolic EVOO that has been stored in ways that protect those polyphenols.
FAQs
Why does high-phenolic EVOO work better than regular olive oil?
High-phenolic extra virgin olive oil tends to work better because its bioactive compounds act on lipid signaling pathways tied to metabolic health.
Put simply, these phenolic compounds don't just sit in the background. They help inhibit HMG-CoA reductase, activate the AMPK pathway, improve LDL uptake, support cholesterol regulation, and strengthen HDL’s antioxidant and anti-inflammatory function.
How much olive oil should I use each day for heart benefits?
Research points to about 1.5 tablespoons (20 grams) of high-phenolic extra virgin olive oil per day to support heart health and metabolic function.
Even a small bump may help. Adding 5 grams a day has been linked to a 4% lower risk of cardiovascular disease.
That said, the strongest effects show up at 20 grams.
Does olive oil lower cholesterol, or mainly protect LDL from oxidation?
Olive oil can help on both fronts.
It may lower LDL cholesterol by affecting the LDLR pathway and inhibiting HMGCoAR activity. In plain English, that means it can help cut down the body’s own cholesterol production.
It can also help protect both LDL and HDL from oxidative damage, thanks to its polyphenols, including hydroxytyrosol and tyrosol. Those same compounds may support HDL function by improving cholesterol efflux.