
Olive Oil Phenols and Lipid Metabolism
If you want the short answer: high-phenol extra virgin olive oil seems to affect oxidized LDL more often than it changes your standard cholesterol numbers.
Here’s the plain-English version:
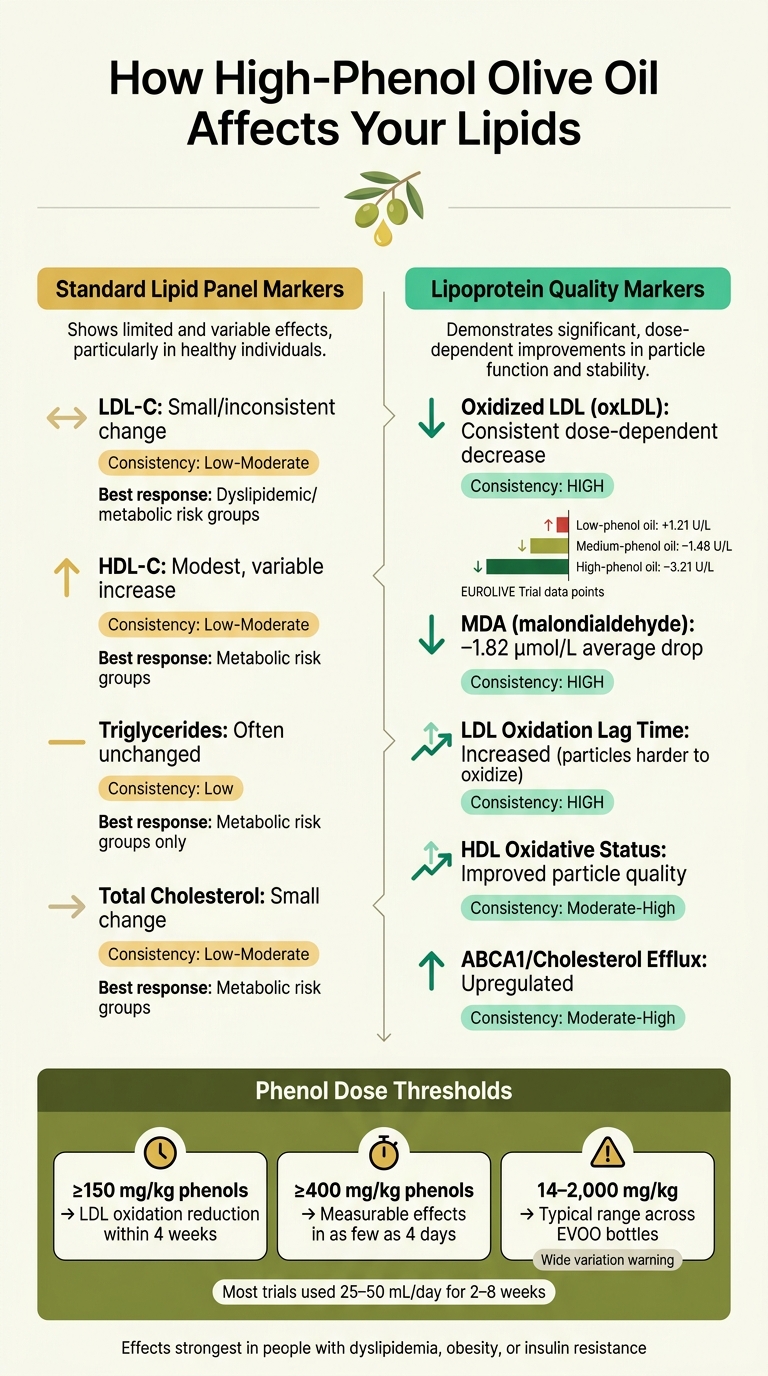
- LDL oxidation drops most often. In trials, high-phenol EVOO lowered oxLDL more steadily than it lowered LDL-C.
- Standard lipid panel changes are usually small. LDL-C, HDL-C, and triglycerides often shift only a little, especially in healthy adults.
- People with metabolic issues may see more movement. Those with dyslipidemia, obesity, or insulin resistance tend to show bigger changes in LDL-C, total cholesterol, triglycerides, and oxLDL.
- Dose matters. Many studies used 25–50 mL/day for 2–8 weeks. Oils with 150 mg/kg+ phenols showed effects on LDL oxidation, and 400 mg/kg+ may act within days.
- The mechanism goes beyond fat type. Olive phenols appear to affect HMG-CoA reductase, AMPK, SREBP, LDL receptors, and cholesterol efflux pathways.
- HDL function may improve even when HDL-C barely changes. Some studies found better cholesterol efflux and more ABCA1/ABCG1 activity.
- Not all EVOO is the same. Phenol content can range from about 14 to nearly 2,000 mg/kg, so one bottle may act very differently from another.
A few numbers stand out. In the EUROLIVE trial, oxLDL changed by +1.21 U/L with low-phenol oil, −1.48 U/L with medium-phenol oil, and −3.21 U/L with high-phenol oil. A 2023 meta-analysis also found average drops of −0.29 U/L in oxLDL and −1.82 μmol/L in MDA.
So when I boil the article down, the main point is simple: olive oil phenols seem to do more for lipoprotein quality and oxidation than for big changes on a routine lipid panel. The rest of the article explains how that happens and where the human evidence is stronger or weaker.
The Best Food for Healthy Cholesterol? Science Says It Might Be Olive Oil
sbb-itb-4066b8e
Human Trial Evidence on Cholesterol and Blood Lipids
High-Phenol EVOO: Lipid Panel vs. Lipoprotein Quality Effects
When you look past lab markers and into human trials, one pattern stands out: high-phenol EVOO lowers oxidized LDL more dependably than it changes LDL-C, HDL-C, or triglycerides.
Results for LDL-C, HDL-C, Triglycerides, and Oxidized LDL
Across controlled trials and meta-analyses, oxidized LDL (oxLDL) is the marker that responds most often to higher-phenol olive oil. The EUROLIVE study is a good example. Healthy men consumed about 25 mL/day of olive oils with low, medium, or high phenolic content over three-week periods. The average oxLDL changes moved in step with phenol content: +1.21 U/L with low-phenol oil, −1.48 U/L with medium-phenol oil, and −3.21 U/L with high-phenol oil.
A 2023 meta-analysis on oxidative stress markers found much the same pattern. It reported weighted mean differences of −0.29 U/L for oxLDL and −1.82 μmol/L for malondialdehyde (MDA), with bigger drops at higher phenol concentrations. LDL-C told a different story. A separate 2023 meta-analysis of 10 randomized controlled trials found only a borderline overall drop in LDL-C, and the effect reached significance only at the highest phenol exposures studied. HDL-C went up a little across trials, while total cholesterol and triglycerides did not change in a steady way.
Some HDL-focused trials add an extra layer here. They show better cholesterol efflux and higher ABCA1/ABCG1 expression, which points to better HDL function rather than a big jump in HDL-C itself.
How Study Populations Affect Results
Study population makes a big difference. In healthy adults with normal baseline lipids, shifts in LDL-C, HDL-C, and triglycerides are often small or missing, even when oxLDL drops by a noticeable amount.
In people with metabolic risk factors like dyslipidemia, insulin resistance, or obesity, the pattern changes. Trials and meta-analyses in these groups show more steady drops in LDL-C, total cholesterol, triglycerides, and oxLDL than studies in healthy volunteers. Age may matter too. Age-stratified data suggest that younger adults, such as those around 35–50 years old, may see clearer drops in oxidized LDL than older participants.
Dose and timing matter as well. Most trials use 25–50 mL per day, or about 2–3 tablespoons, for 2–8 weeks. Oils with at least about 150 mg/kg total phenols can lower LDL oxidation within four weeks, and oils above 400 mg/kg may show measurable effects in as little as four days.
Clinical Study Patterns by Outcome: Comparison Table
| Outcome | Consistency | Most Responsive Group | Phenol Level Linked to Effect |
|---|---|---|---|
| Oxidized LDL (oxLDL) | High - most reliable finding | Healthy adults and metabolic risk groups | ≥150 mg/kg; stronger at >300–400 mg/kg |
| Malondialdehyde (MDA) | High | Both healthy and at-risk populations | Moderate to high phenol exposure |
| HDL function (efflux capacity) | Moderate-high | Healthy adults | Moderate phenol exposure |
| HDL-C | Modest, variable | Metabolic risk groups | High daily polyphenol exposure |
| LDL-C | Low-moderate; often small | Dyslipidemic or metabolic risk groups | Highest phenol exposures studied |
| Total cholesterol | Low-moderate | Metabolic risk groups | High phenol exposure |
| Triglycerides | Low - inconsistent | Metabolic risk groups | Unclear; often unchanged |
Taken together, these study patterns line up more with changes in oxidation and HDL behavior than with big shifts in standard lipid panel numbers. They also point toward changes in HMG-CoA reductase, AMPK, and related lipid pathways.
Enzyme and Pathway Effects Linked to Olive Oil Phenols
Human trial data help explain why olive oil phenols tend to lower oxLDL more consistently than standard lipid markers. The story isn’t just about total cholesterol or LDL-C. It also involves the enzymes and signaling pathways that shape how cholesterol is made, handled, and protected from oxidation.
HMG-CoA Reductase, ACAT, and LDL Receptor Activity
HMG-CoA reductase (HMGCoAR) is the rate-limiting enzyme in cholesterol synthesis. Studies in HepG2 human liver cells found that EVOO phenol extracts inhibit this enzyme in a dose-dependent way, which lowers cholesterol synthesis inside the cell. The phenols most tied to this effect are secoiridoid derivatives of hydroxytyrosol and tyrosol, including oleuropein aglycone and ligstroside derivatives.
As intracellular cholesterol falls, liver cells respond by increasing LDL receptor (LDLR) protein levels, which helps clear more LDL from circulation. This shift is driven by SREBP-2. In HepG2 cells treated with 25 µg/mL of EVOO phenol extract, SREBP-2 activation increased LDL uptake. Animal work on polyphenol-rich diets shows the same general pattern: lower hepatic HMGCoAR activity, higher LDL receptor levels, and less VLDL secretion. That lines up with the broader effects seen on AMPK and liver fat synthesis.
Direct evidence for ACAT is still thin. Most papers infer an effect based on changes in intracellular cholesterol and LDLR activity rather than direct ACAT measurements.
AMPK, SREBP, and Control of Lipogenesis
AMPK phosphorylation increased in HepG2 cells exposed to EVOO phenol extracts, which inhibited both HMGCoAR and acetyl-CoA carboxylase (ACC), another rate-limiting enzyme, this time in fatty acid synthesis. In primary rat hepatocytes, 25 µM hydroxytyrosol reduced ACC activity by 41%, oleuropein by 38%, and tyrosol by 17% within 2 hours. In that same window, HMG-CoA reductase and diacylglycerol acyltransferase (DGAT) activity also fell by a clear margin.
AMPK activation also suppresses SREBP-1c, a main driver of lipogenesis. SREBP-1c controls the expression of genes such as fatty acid synthase (FASN) and ACC, while SREBP-2 increases LDLR expression. Put simply, this means less new fatty acid production, lower triglyceride output, and less fat buildup in the liver. That matters even more in insulin resistance or high-carbohydrate diet settings, where lipogenesis tends to run high.
Oleuropein also acts as a PPAR-α agonist, which supports fatty acid oxidation and improves hepatic lipid handling. So the same phenols that slow cholesterol synthesis also help limit oxidative damage to LDL.
Mechanism Map: Enzymes, Signals, and Lipid Effects
The table below connects the signaling changes with enzyme targets and lipid outcomes.
| Level | Key Players | Downstream Effect |
|---|---|---|
| Signaling | AMPK↑, PPAR-α↑, SREBP-1c↓, NF-κB↓ | Reduced lipogenic gene expression; enhanced fat oxidation |
| Enzyme targets | HMGCoAR↓, ACC↓, FASN↓, DGAT↓, LDLR↑ | Lower cholesterol and fatty acid synthesis; better LDL uptake |
| Lipid outcomes | Cholesterol synthesis↓, triglycerides↓, LDL-C↓, oxLDL↓ | Improved blood lipid profile; reduced cardiovascular risk markers |
Hydroxytyrosol and oleuropein show the strongest effects at the enzyme level, but that’s only part of the picture. Those same signals also shape LDL oxidation and HDL-mediated cholesterol transport, which helps explain why olive phenols affect oxLDL and HDL function, not just LDL production.
Oxidation, HDL Function, and Cholesterol Transport
Why Oxidized LDL Matters Beyond LDL Quantity
Those enzyme shifts help explain something a basic lipid panel can miss: olive oil phenols affect lipoprotein quality, not just lipid output. A standard U.S. lipid panel shows LDL cholesterol in mg/dL, but the state of LDL matters just as much as the amount. Oxidized LDL (oxLDL) is taken up much more easily by macrophages in artery walls, which speeds up plaque buildup and inflammation - even when LDL-C is only moderately high.
High-phenolic EVOO consistently lowers oxLDL and increases LDL oxidation lag time. Put simply, the particles become harder to oxidize. Phenols like hydroxytyrosol and related secoiridoids attach to LDL particles, where they help neutralize reactive oxygen species and steady the particle against lipid peroxidation.
One human enrichment study showed just how much this can matter. LDL had 1.75-fold to 14.58-fold reductions in conjugated diene formation depending on the level of polyphenol enrichment. That points to a direct link between phenolic content in the oil and measurable particle-level protection. In plain English: not all olive oil works the same here. The phenol load plays a big part in how much protection shows up.
HDL Function, ABCA1 Activity, and Cholesterol Efflux
EVOO polyphenols may also help HDL do its job better by increasing ABCA1 and related transport pathways involved in cholesterol efflux. Phenol-rich oils also support efflux through ABCG1 and SR-BI, which work with more mature HDL particles. This fits with the AMPK/SREBP shifts discussed above by improving how cholesterol is handled after production.
In the same human enrichment study, HDL showed 4.53-fold to 7.71-fold reductions in conjugated diene formation after polyphenol enrichment. That means the HDL particles themselves became more resistant to oxidative damage, which matters because particle structure affects how well HDL interacts with efflux transporters.
That said, the data don't line up perfectly across every trial. One randomized crossover study found that EVOO improved the HDL lipid fraction without a measurable increase in cholesterol efflux capacity. So the HDL may change first, while function takes longer to shift - or may not shift the same way in every study design.
That’s why lipid quantity and lipoprotein quality need to be looked at as separate issues.
Lipid Levels vs. Lipoprotein Quality: Comparison Table
The table below separates what standard lipid panels measure from what lipoprotein quality markers show, and how olive oil phenols tend to affect each.
| Outcome Category | Specific Marker | Effect of High-Phenolic EVOO |
|---|---|---|
| Standard lipid panel markers | LDL-C, HDL-C, triglycerides | Modest or inconsistent change |
| Lipoprotein quality | Oxidized LDL (oxLDL) | Consistent, dose-dependent decrease with higher phenolic content |
| Lipoprotein quality | LDL oxidation lag time | Increased, indicating greater resistance to oxidative damage |
| Lipoprotein quality | HDL oxidative status | Improved; reduced oxidative modification of apoA-I and phospholipids |
| Reverse cholesterol transport | ABCA1 activity / cholesterol efflux | Upregulated in mechanistic and human studies; not uniform across all trials |
A near-normal LDL-C result can still mask a heavy oxLDL burden, and high-phenolic EVOO appears to act on that part of the picture even when standard lipid numbers move only a little.
What the Evidence Means for EVOO Quality and Key Takeaways
Why Phenol Content Varies Across Extra Virgin Olive Oils
If the strongest trial results depend on phenol dose, then EVOO quality becomes the thing that matters most.
Phenolic content in EVOO can range from about 14 to nearly 2,000 mg/kg, based on how and when the oil was produced. That's not a small gap. It's big enough to change the biological effect you get from the oil. Put simply, an EVOO with very low phenol content may not deliver the same LDL-oxidation benefits seen in higher-phenol oils.
A few factors explain most of that spread:
- Harvest timing: Early-harvest olives usually have more phenols than fully ripe olives.
- Cultivar: The olive variety makes a difference.
- Processing: Cold extraction below about 80°F / 27°C and limited water contact help keep water-soluble phenols in the oil.
- Storage: Light, heat, and oxygen lower phenol levels over time.
So an oil that sits around too long, or is stored badly, can end up far below the phenolic levels used in trials that showed strong results.
This also helps explain why studies don't always line up neatly. Two trials may both test "extra virgin olive oil", but if the phenol content is very different, the outcomes can be different too.
Limits of Current Research
The evidence is good, but it has clear limits.
Most human trials are small, often with fewer than 50 participants, and many last only 3 to 8 weeks. That's long enough to pick up changes in oxidized LDL, but not long enough to track hard cardiovascular outcomes like heart attacks or strokes.
There's another issue: the phenols themselves aren't tested in the same way across studies. Some trials use isolated hydroxytyrosol. Others use whole EVOO with mixed phenolic profiles. Those are not apples-to-apples comparisons.
The study groups also differ a lot. Some include healthy adults, while others include people with stable heart disease. Many are done in the setting of a Mediterranean-style diet, which makes it harder to apply the findings to other eating patterns.
Conclusion: Main Points from the Research
Taken together, these quality differences help explain why changes in oxLDL look more steady than changes in a standard lipid panel.
Oxidized LDL stands out as the most reliable target. High-phenolic EVOO lowers it in a dose-dependent way, and that link appears tied to phenolic content itself, not just olive oil in general. A 2023 dose-response review found a linear link between higher phenol content and lower oxLDL and MDA.
By contrast, standard lipid panel markers like LDL-C, HDL-C, and triglycerides tend to move only a little, or not in a consistent direction. The clearer signal seems to be in lipoprotein quality: how well LDL resists oxidation and how well HDL supports cholesterol efflux.
Mechanistic data also point to effects on HDL function and ABCA1-mediated cholesterol transport, but the human evidence on exact enzyme-level pathways is still limited. In plain terms, the label alone doesn't tell you much. Phenolic content is what shapes the size of the effect.
FAQs
How can I tell if an EVOO is high in phenols?
Look for labels like early harvest or high-phenolic. They often point to at least 250 mg/kg of polyphenols. Processing matters here, too. Go with high-quality, cold-pressed extra virgin olive oil, since refined oils contain almost none.
To get more from the oil, pick options with higher polyphenol levels and use them raw when you can. That helps protect their properties.
Do olive oil phenols help if my cholesterol is normal?
Yes. Even if your cholesterol numbers look normal, olive oil phenols may still help. Their main role is to protect LDL from oxidative damage, which matters because oxidized LDL can contribute to plaque buildup.
They may also help improve HDL function and lower inflammation. That supports heart health and helps the body move cholesterol where it needs to go.
How much high-phenol EVOO was used in studies?
Amounts varied from one study to another. Clinical trials often used 25 milliliters per day - about 1.7 US tablespoons. Some studies went lower, with amounts such as 8 grams per day.
In broader heart health research, including PREDIMED, participants consumed about 3.5 to 4.3 US tablespoons per day. Oils with higher phenolic levels - ranging from 366 to 1,021 mg/kg - were linked to stronger cardiovascular benefits.